
The Capnography Detective - Mastering End-Tidal CO2 Monitoring
What is your understanding of capnography? If you think it is just something to confirm ETT placement you couldn’t be more wrong. Monitoring carbon dioxide levels is an essential tool for assessing respiratory function and guiding patient care.
The CO2 Detective
Imagine end-tidal CO2 (ETCO2) monitoring as a detective game. Your patient's exhaled breath holds the clues to their respiratory and cardiovascular status. It's like solving a mystery, but instead of fingerprints, you're analysing carbon dioxide levels. Who knew monitoring could be so thrilling?
The Normal ETCO2 Range
Our normal ETCO2 should range from 35-45 mmHg and closely match the partial pressure of CO2 in the bloodstream (PaCO2). Anything above or below these ranges, or where there is significant difference between ETCO2 and PaCO2 should prompt us to grab our detective hats to investigate what the cause is.
Investigating High or Low ETCO2 Levels
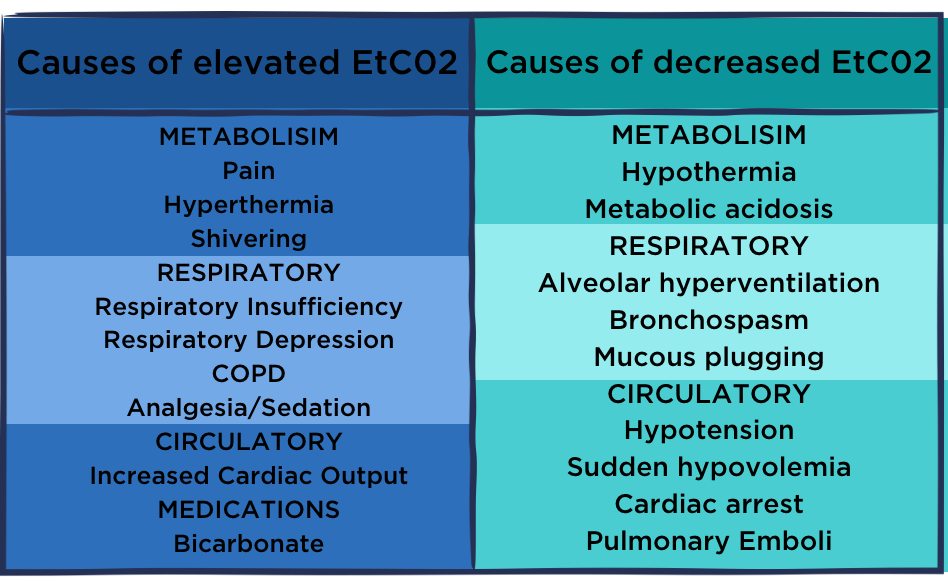
High levels may indicate hypoventilation, while low levels may suggest hyperventilation or inadequate perfusion. It's important to approach your investigation systematically starting with your patient and their equipment to determine if changes in those are contributing to the high or low levels. For example a patient who is spontaneously ventilating, but has just been administered an anaesthetic and is developing a respiratory depression as a result - we would expect their ETCO2 to rise as their respiratory rate reduces. See Table 1 for Patient Factors that Effect CO2.
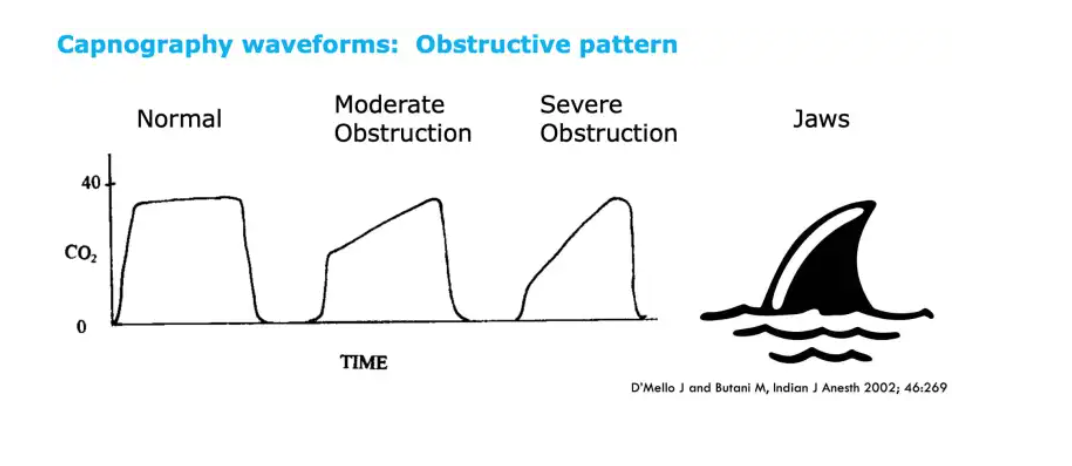
Analysis of the waveform shape and pattern, also tells a story. Looking for abnormalities such as a sudden decrease or increase in ETCO2, which may indicate changes in respiratory or circulatory function. ETCO2 waveform can also provide insights into the effectiveness of cardiopulmonary resuscitation (CPR) efforts. Lastly, evaluation of shape of the ETCO2 waveform helps identify conditions like bronchospasm, airway obstruction, or equipment malfunctions.
For example a mild obstruction such as due to COPD or asthma increases the slope of the wave form, whilst a larger obstruction due to a partially obstructed airway such as in anaphylaxis or laryngospasm may cause the wave form to appear very sloped like a shark fin.
If you notice your patient’s ETCO2 deviating from the normal range, it’s leaving you clues regarding their respiratory function, ventilation and perfusion status. Get curious and investigate the reason why and use capnography to ensure patient safety and optimise outcomes.
Further Learning
Explore further in our critical care update webinar The vital role of haemodynamic monitoring in the critically ill patient.
Join us in our Lunch and Learn: Capnography session, which will provide top tips to demystify capnography and help recognise the vital role it plays in providing effective treatment and enhancing patient safety.
References

Grace Larson, RN, BN, CertIV(TAE), GradDipClinNurs(PaedCritCare), MAdNursPrac(PaedCritCare), has extensive experience in paediatric nursing, with 13 years in Paediatric Intensive Care Units (PICU). She’s published journal articles in the specialty area of pain and sedation in PICU, and has presented at national and international conferences on the area of pain and sedation in paediatrics. Grace has previously worked with the ACCCN delivering Paediatric Advanced Life Support in Victoria, bringing a wealth of experience into her clinical teaching on paediatric resuscitation. She has also consulted with NSW Health on quality and safety delivering within PICU, and has been contracted with the ANMF to develop nursing programs for nurses who require additional education as part of their practice requirements.
Become a member and get unlimited access to 100s of hours of premium education.
Learn moreFollow James, a 7-year-old boy scheduled for a tonsillectomy and adenoidectomy, as we explore how the 4 P’s of child preparation – Prepare, Play, Parent, Praise – can be used in day surgery to reduce procedural anxiety, support family-centred care, and improve the overall patient experience
Caregiver concern is a powerful predictor of clinical deterioration in children, often surpassing abnormal vital signs. A recent Lancet study confirms its association with ICU admission and ventilation. Integrating caregiver input into assessments, documentation, and escalation protocols can significantly improve early recognition and outcomes in paediatric emergency care.
Seeking guidance on which courses to prioritise before the CPD year concludes? You're not alone! Essential CPD for Australian nurses covering skills, patient care & standards.