
Beth presents with sudden onset chest discomfort - Clinical Opal
Beth is a 52 year old musician who presents complaining of sudden onset chest discomfort. She describes the pain as a heavy pressure in the centre of her chest that radiates to her left arm. She also reports feeling nauseous and sweaty.
Beth has a history of asthma that is well controlled. She is a non-smoker and leads a moderately active lifestyle.
Beth is pale & diaphoretic, BP 160/90, HR 90 and regular, SpO2 96% on room air.
Should a 12 lead ECG be prioritised for Beth?
Yes. Prioritising a 12 lead ECG when a patient presents with symptoms suggestive of acute coronary syndrome (ACS) is crucial for several reasons:
-
Differentiating causes of chest pain - ACS encompasses a spectrum of conditions including ST elevation myocardial infarction (STEMI), and non-ST elevation infarcts (NSTEACS).
-
Time to diagnosis - Time is tissue in ACS management especially in cases of STEMI or LBBB infarcts where rapid reperfusion via percutaneous coronary intervention (PCI) or fibrinolysis is required. A 12 lead ECG allows for prompt diagnosis, reducing door-to-balloon times for patients requiring PCI
-
Risk stratification - The findings from a 12 lead ECG aid in risk stratification and guide subsequent management decisions including the need for immediate reperfusion therapy, or further investigations such as cardiac biomarkers and clinical risk scores such as HEART
-
Communication - a 12 lead ECG provides a documented record of the patient’s current cardiac status. This is an important part of communication between healthcare workers including GP-Paramedic-ED-Cardiologist. Serial ECGs, and ECGs performed during chest pain episodes also assists diagnostic processes and provides a valuable reference for ongoing management and follow up care.
A 12 lead ECG was performed on Beth.
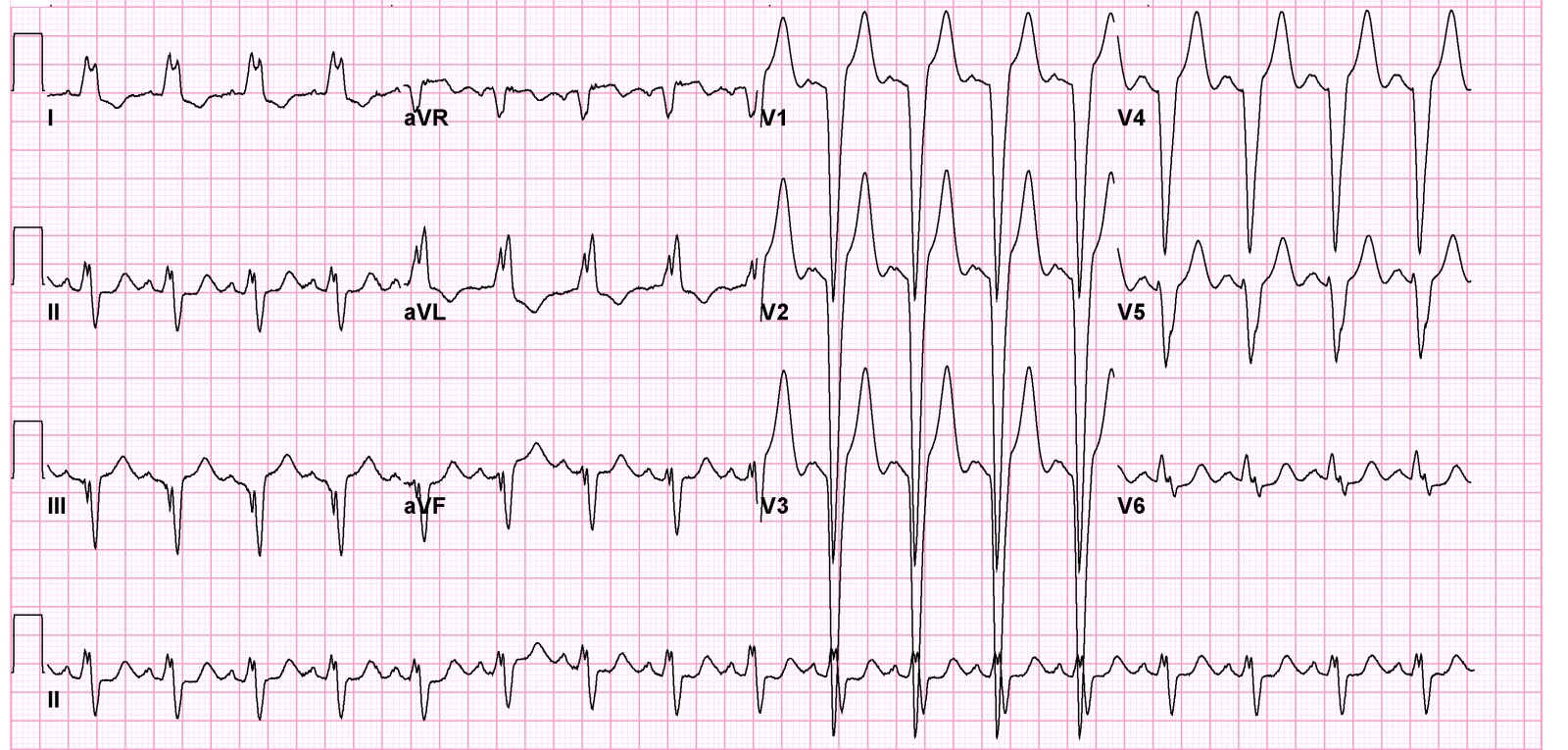
What is your interpretation? Is the ECG showing any axis deviation? Will this be significant in Beth’s care? What other assessment/investigations would you do on Beth to support your diagnosis and treatment plan?
You can find out all the answers in our ECG Interpretation course.
Related courses
ECG Interpretation Course
Emergencies in General Practice Course
Advanced Life Support Course
The ALERT Course

Ken Hambrecht RN, ICU Cert., B.Sc, (Physiology & Biochem.), M.I.Biol, M.Ed., J.P. MACN, has extensive experience in Critical Care practice & Medical education. This includes more than 25 years co-ordinating & teaching Critical Care Courses and other Medical Education. Ken is the Founder and Principal Consultant for Critical Care Education Services.
In recognition of his outstanding contribution to medical education, Ken has been awarded honorary life membership of the Australian College of Perianaesthesia Nurses (ACPAN). Ken has also been a member of the Australian Resuscitation Council, including the Advanced Life Support Committee.
Become a member and get unlimited access to 100s of hours of premium education.
Learn moreFollow James, a 7-year-old boy scheduled for a tonsillectomy and adenoidectomy, as we explore how the 4 P’s of child preparation – Prepare, Play, Parent, Praise – can be used in day surgery to reduce procedural anxiety, support family-centred care, and improve the overall patient experience
Caregiver concern is a powerful predictor of clinical deterioration in children, often surpassing abnormal vital signs. A recent Lancet study confirms its association with ICU admission and ventilation. Integrating caregiver input into assessments, documentation, and escalation protocols can significantly improve early recognition and outcomes in paediatric emergency care.
Seeking guidance on which courses to prioritise before the CPD year concludes? You're not alone! Essential CPD for Australian nurses covering skills, patient care & standards.