
‘When in ROME’ ABG interpretation - Clinical OPAL
Jane, a 28-year-old woman, is admitted to the surgical ward following an emergency appendectomy.
She is receiving a Morphine infusion at 3 mg/hr along with regular paracetamol.
Post-operatively, she remains drowsy and difficult to wake, an arterial blood gas (ABG) has been obtained.
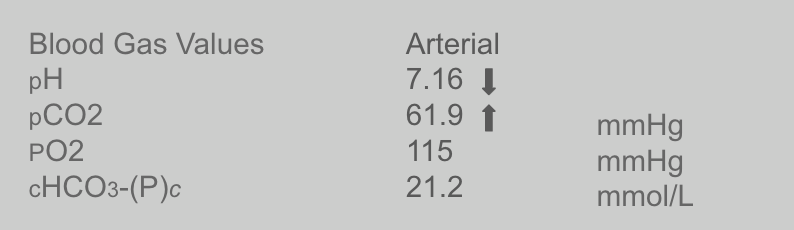
What is your interpretation of Jane’s ABG, and what is the main cause?
Answer
Respiratory Acidosis likely from CO₂ retention due to narcosis.
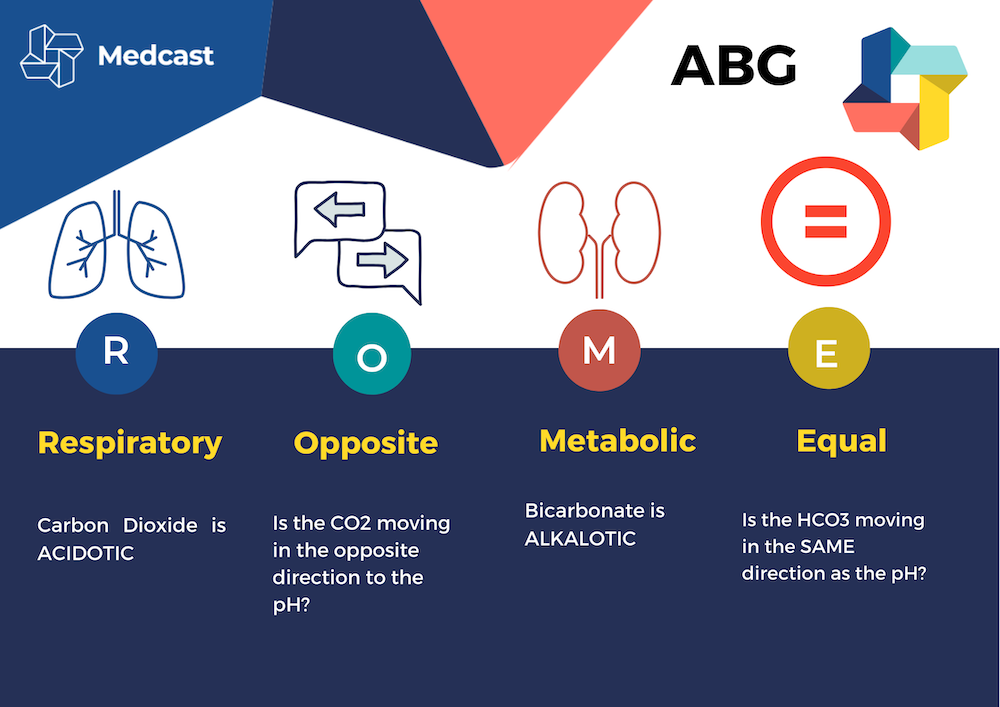
ROME ABG Interpretation Mnemonic
The ROME mnemonic is a helpful tool for interpreting arterial blood gas (ABG) results, particularly in assessing acid-base balance.
Respiratory (R): This refers to the primary process affecting the pH due to changes in the partial pressure of carbon dioxide (PaCO2) in the blood. If the PaCO2 is abnormal it is either a primary respiratory cause or indicates compensation via the respiratory system.
Opposite (O): This indicates the direction of change in the pH and PaCO2. If the pH and PaCO2 move in opposite directions, it suggests a respiratory cause of the acid-base imbalance.
Metabolic (M): This refers to the renal process affecting the pH due to changes in the bicarbonate (HCO3) levels in the blood. If the bicarbonate level is abnormal, it is either a primary metabolic cause or indicates compensation via the renal buffering system.
Equal (E): This indicates the direction of change in the pH and bicarbonate levels. If the pH and bicarbonate levels move in the same direction, it suggests a metabolic cause of the acid-base imbalance.
In this case study, arterial blood gas analysis using the ROME ABG mnemonic reveals respiratory acidosis in a postoperative patient with no compensation. Prompt identification and management of respiratory depression is crucial to prevent further complications and promote optimal patient outcomes.
Jane’s Morphine infusion should be paused and a dose of naloxone administered to reverse the respiratory depression, a review of her opioid requirements should also be performed.
Related courses

Grace Larson, RN, BN, CertIV(TAE), GradDipClinNurs(PaedCritCare), MAdNursPrac(PaedCritCare), has extensive experience in paediatric nursing, with 13 years in Paediatric Intensive Care Units (PICU). She’s published journal articles in the specialty area of pain and sedation in PICU, and has presented at national and international conferences on the area of pain and sedation in paediatrics. Grace has previously worked with the ACCCN delivering Paediatric Advanced Life Support in Victoria, bringing a wealth of experience into her clinical teaching on paediatric resuscitation. She has also consulted with NSW Health on quality and safety delivering within PICU, and has been contracted with the ANMF to develop nursing programs for nurses who require additional education as part of their practice requirements.
Become a member and get unlimited access to 100s of hours of premium education.
Learn moreFollow James, a 7-year-old boy scheduled for a tonsillectomy and adenoidectomy, as we explore how the 4 P’s of child preparation – Prepare, Play, Parent, Praise – can be used in day surgery to reduce procedural anxiety, support family-centred care, and improve the overall patient experience
Caregiver concern is a powerful predictor of clinical deterioration in children, often surpassing abnormal vital signs. A recent Lancet study confirms its association with ICU admission and ventilation. Integrating caregiver input into assessments, documentation, and escalation protocols can significantly improve early recognition and outcomes in paediatric emergency care.
Seeking guidance on which courses to prioritise before the CPD year concludes? You're not alone! Essential CPD for Australian nurses covering skills, patient care & standards.