
Physical Assessment Techniques for ICU Nurses: Identifying and managing patient deterioration - Clinical Opal
You’ve come on shift and have been allocated to Carl, a 53 year old gentleman who was admitted to the ICU 2 weeks ago with community acquired pneumonia and sepsis.
Carl has required mechanical ventilation, renal replacement therapy and vasopressor support. He had a tracheostomy inserted 5 days ago and is now being weaned off the ventilator, currently on pressure support ventilation (PSV) with a PEEP of 5 and PS of 15.
Today he is agitated and confused, his urine output has dropped.
Question
What assessment should you perform to determine the cause of Carl’s deteriorating state?
Answer
Physical assessments in the intensive care unit (ICU) are fundamental to patient care, but the process can be notably different from standard procedures used in general acute care settings. For ICU nurses, understanding these differences is crucial for effectively monitoring and managing critically ill patients.
The unique nature of ICU patients, often marked by complex conditions and the presence of life-supporting devices, necessitates adaptations in standard assessment approaches. According to a study published in the American Journal of Critical Care, ICU patients typically exhibit higher acuity levels, requiring more specialised and frequent assessments compared to general ward patients.
Our priority for patients like Carl is pinpointing the source of deterioration. The most effective tool for ICU nurses in this regard is a rapid, comprehensive bedside assessment. This assessment, crucial at the start of a shift, after breaks, and during any change in patient condition, gives a snapshot of the patient's stability, the level of support they're receiving, and the current care plan.
Physical assessments in the ICU usually involve a primary and secondary survey. The primary survey follows the ABCDE (Airway, Breathing, Circulation, Disability, Exposure) approach, a method supported by 87% of critical care nurses as per a survey in Critical Care Nursing Quarterly. The secondary survey involves a detailed, systems-based evaluation from head to toe. When drilling down to a specific area of concern, the tertiary survey employs specific assessment tools.
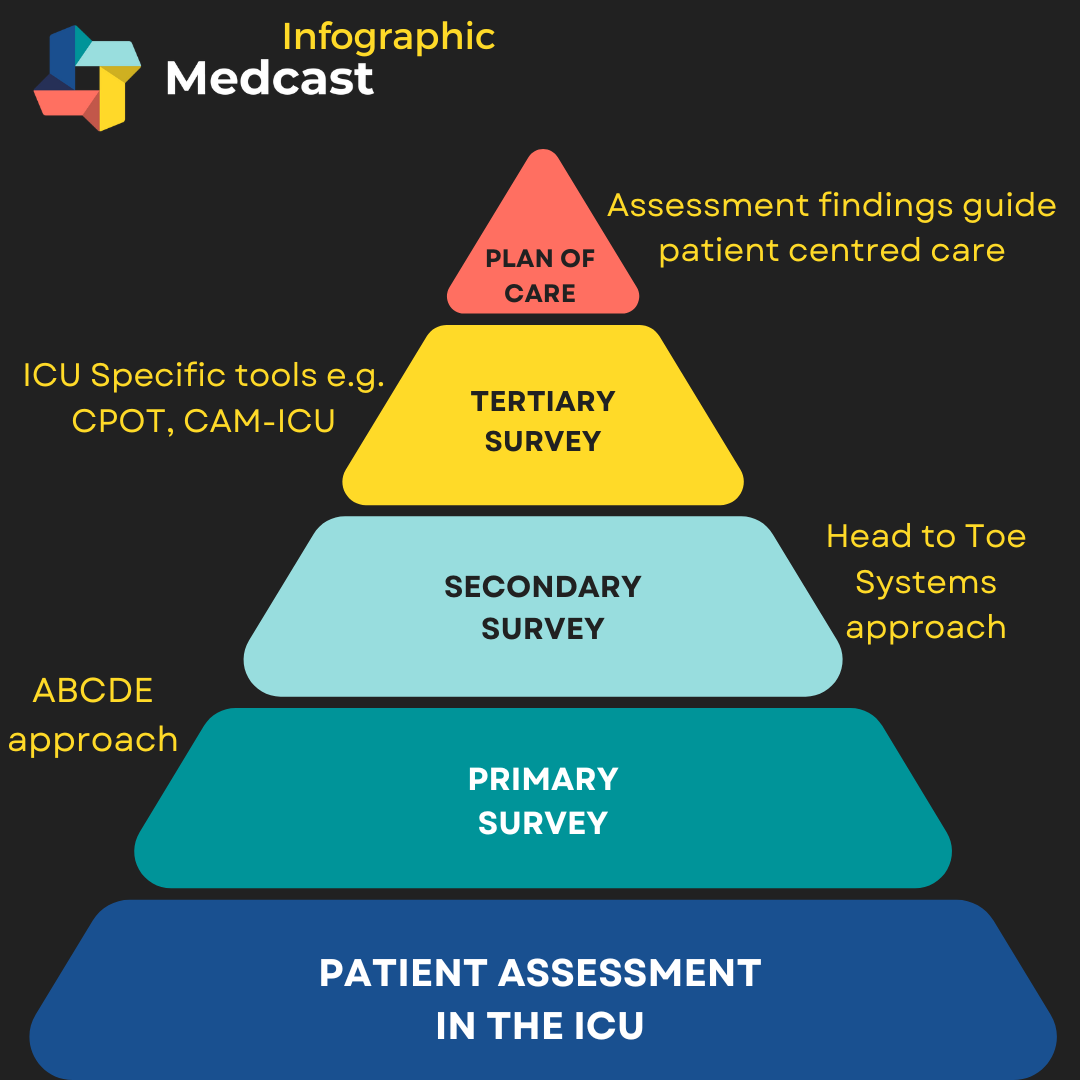
When assessing patients, it's vital to start from the patient and work outward. Begin with a direct physical assessment, then evaluate monitoring and treatment devices, and finally, review recent results like arterial blood gases (ABG) and x-rays. During periods of deterioration or to evaluate treatment responses, more specific tools may be necessary.
For instance, in Carl’s case, an ABCDE assessment followed by a head-to-toe survey is essential. Given his deterioration, exploring changes in renal function can be pivotal to understand if his confusion stems from sepsis, poor renal clearance and uraemic encephalopathy, or ICU-related delirium.
In the ICU, utilising specific assessment tools such as the Critical-Care Pain Observation Tool (CPOT) for pain assessment or the Confusion Assessment Method for the ICU (CAM-ICU) can be instrumental. These tools help gather critical data for managing pain, agitation, and delirium, enhancing patient care. A 2022 study in the Journal of Clinical Nursing highlighted the effectiveness of these tools in improving patient outcomes in ICUs.
By integrating these specialised assessment techniques and tools, ICU nurses can more accurately identify patient deterioration and tailor interventions effectively, ultimately improving patient outcomes in the critical care setting.
Related courses

Susan is the Head of Nursing Education for the Medcast Group.
DipAppScNsg, BN, CritCareCert, CoronaryCareCert, TraumaNsgCareCert, CertIV(TAE), MN(Ed), and GradCert(Ldrshp & Mgt).
Become a member and get unlimited access to 100s of hours of premium education.
Learn moreMarjory is a 68 year old in-patient who is 2 days post hip replacement. She is on rivaroxaban (xarelto) for VTE prophylaxis. You find her sitting on the floor of the bathroom, alert but in pain.
We explore the case of Edward, a patient with acute kidney injury (AKI), focusing on renal protection strategies. It explores fluid management, blood pressure control, nephrotoxic drug adjustments, and electrolyte monitoring. Treatment considerations include vasoactive medications, dialysis options like CRRT, and medication dosing to support renal recovery and prevent complications.
James, a university student with a history of seasonal allergic rhinitis, presents with sudden respiratory distress following exposure to grass pollen during a soccer game shortly before a summer thunderstorm. Could this be thunderstorm asthma?