
Non-invasive prenatal testing/screening (NIPT/S) - clinical fact sheet and MCQ
![]()
Overview
Non-invasive prenatal testing/screening (NIPT/S) is a screening test which is available from 10 weeks’ of pregnancy. Cell-free DNA (cfDNA) from the placenta crosses into the pregnant parent’s bloodstream and can be tested to check for certain chromosomal conditions [1]. The main chromosomal conditions which standard NIPT/S screen for are:
- trisomy 21 (Down syndrome)
- trisomy 18 (Edward syndrome)
- trisomy 13 (Patau syndrome)
- differences in the sex chromosomes (X and Y)
Chromosomal conditions can occur in the following ways:
- aneuploidy: a difference in the expected number of chromosomes (ie a whole extra or missing chromosome), which is the type of chromosome condition screened for in the standard NIPT panel
- copy number variants (CNVs): are microdeletions and microduplications of chromosomes (ie small, partial extra or missing pieces of chromosome)
- segmental aneuploidies: are deletions and duplications of chromosomes (ie large, partial extra or missing pieces of chromosome)
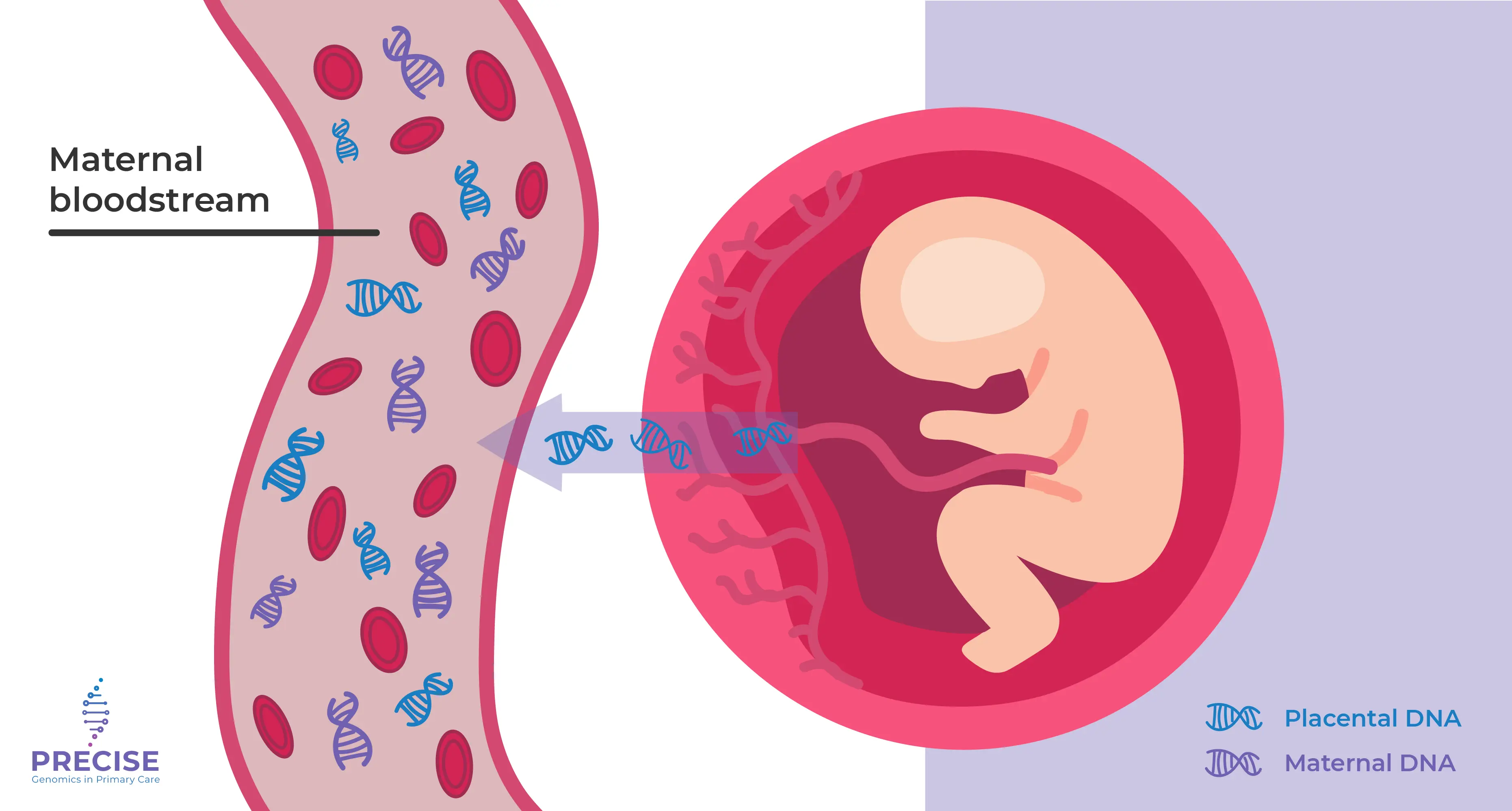
Image 1: cell free DNA from the placenta can cross into the maternal blood stream
(source: PRECISE Genomics)
Who can be offered NIPT/S?
- All patients can be offered NIPT/S as a primary aneuploidy screening test from 10 weeks’ gestation
- If a patient declines NIPT/S but would still like aneuploidy screening, combined first trimester screening (cFTS) is the recommended screening option. This involves measuring nuchal translucency (NT) in the foetus by ultrasound, and maternal blood pregnancy-associated plasma protein-A (PAPP-A) and free beta-hCG
- If there is an intermediate or high probability cFTS result, NIPT/S can also be offered as a contingent aneuploidy screening test
NIPT/S can be ordered directly through most private pathology companies. Some hospitals and specialist women’s health ultrasound providers will also offer NIPT/S.
When should NIPT/S be offered?
NIPT/S should be offered from 10 weeks’ gestation. A dating scan is performed prior to NIPT/S to confirm foetal viability, gestational age, identification of multiple pregnancies, and any major foetal anatomical differences.
NIPT/S should be accompanied by a first trimester anatomy scan at 12-14 weeks and a second trimester anatomy scan at 18-20 weeks to identify any major foetal anatomical differences not visible at the dating scan.
Testing options
1. Standard NIPT/S
- Screens chromosomes 21, 18, 13 as well as chromosomes X and Y
- All currently available NIPT/S platforms perform well for detecting the common autosomal aneuploidies (trisomy 21, 18 and 13) with no significant differences in accuracy
2. Expanded panel NIPT/S
- Screens for a more comprehensive list of chromosomal conditions in addition to the standard NIPT/S
- Can identify:
- CNVs (microdeletions or microduplications)
- 22q11.2 deletion syndrome, also known as velocardiofacial syndrome (VCFS) or Di George syndrome, which is the most commonly screened CNV
3. Genome-wide NIPT/S
- Screens all 23 pairs of chromosomes
- Can identify rare autosomal trisomies (RATs) – the most commonly identified being trisomy 7, 15 or 16
- Can identify large missing pieces of chromosome (known as segmental aneuploidies) across all chromosomes which are of a minimum size (~7Mb in size or greater)
It can be challenging for GPs and patients to choose between standard NIPT/S or an expanded panel, and to identify which pathology provider to use.
The Royal Australian and New Zealand College of Obstetricians and Gynaecologists (RANZCOG) does not recommend an expanded panel or genome-wide NIPT/S for routine population-based screening due to insufficient accuracy [2].
No single pathology provider or testing laboratory is recommended over any other and offerings change frequently. A list of available pathology providers can be found here and is current at the time of publication.
NIPT/S for single genes is not widely available or recommended for routine population-based screening and is only available via a clinical genetics service.
Test contraindications
A number of clinical circumstances exist where a screening test may not be clinically appropriate compared to a prenatal diagnostic test via chorionic villus sampling (CVS) or amniocentesis, which provides definitive testing for a wider range of chromosomal conditions.
These clinical circumstances include:
- significant foetal anatomy differences
- abnormal placental biochemistry:
- Papp-A < 0.2 MoM
- bHCG < 0.2 or > 5 MoM
- known maternal malignancy
- maternal transplant recipient
- triplet or higher order multiple pregnancies
- known parental chromosomal condition
Pre-test counselling includes:
- NIPT/S is optional
- Benefits of NIPT/S:
- test is non-invasive and poses no risk to the pregnant parent or the foetus
- NIPT/S has a higher sensitivity and lower false positive rate than cFTS in both singleton and twin pregnancies
- Limitations of NIPT/S:
- it is a screening test – prenatal diagnostic testing is indicated if a high probability result is returned [3]
- both false positives and false negatives can occur
- test failure can occur due to insufficient cfDNA
- it cannot identify every chromosomal condition
- it is less accurate for multiple pregnancies
- there is no Medicare Benefit Schedule (MBS) rebate available and there is an out-of-pocket cost
- it does not test for carrier status of autosomal recessive or X-linked conditions; reproductive genetic carrier screening (RGCS) is available for this purpose
Post-test counselling
Post-test counselling topics differ based upon the result received.
1. Low probability result:
- provide reassurance, while clearly communicating residual risk
- emphasise the importance of first and second trimester anatomy ultrasounds and standard antenatal care
2. High probability result:
- if a patient receives a high probability result, prenatal diagnostic testing via an amniocentesis is recommended. An amniocentesis can be performed from 15 weeks’ of pregnancy and has a <1% chance of miscarriage associated with the procedure [3]
- occasionally, the chromosomal complement of the placenta can differ from that of the foetus leading to confined placental mosaicism (CPM). Amniocentesis is recommended as it directly tests foetal DNA compared to CVS which uses placental DNA
- referral should be made to a maternal foetal medicine (MFM) service or specialised women’s ultrasound provider to arrange prenatal diagnostic testing
- genetic counselling may also be available via the pathology provider
- if prenatal diagnostic testing confirms a common chromosome condition, and the pregnant person wishes to terminate the pregnancy, this can usually be arranged by the involved MFM service
- if prenatal diagnostic testing confirms a CNV, RAT, or sex chromosome aneuploidy, and the pregnant person requires genetic counselling about this less common chromosome condition, refer your patient to a clinical genetics service
- your patient’s local clinical genetics service can be identified here [4]
- do not refer to clinical genetics before a diagnostic result is available
3. Test failure:
- test failure occurs 2-4% of the time
- if there is insufficient cfDNA (known as low foetal fraction) the test will fail
- low foetal fraction is influenced by gestational age, maternal weight (higher BMI), or maternal medical conditions
- repeating the test at a later gestation may return a result
- if repeat testing also fails, consider other options for aneuploidy screening or diagnosis
4. False positive or false negative results
- False positive and false negative results can occur due to:
- CPM
- unknown maternal sex chromosome aneuploidy
- cfDNA from a demised twin
- maternal malignancies
- maternal organ transplantation recipient
- maternal blood transfusion recipient.
References
- Centre for Genetics Education. Non-Invasive Prenatal Testing. Sydney: NSW Health; 2022. Available from: https://www.genetics.edu.au/PDF/Non_invasive_prenatal_testing_fact_sheet-CGE.pdf. (last accessed August 2025).
- Royal Australian and New Zealand College of Obstetricians and Gynaecologists. Screening and diagnosis of fetal structural anomalies and chromosome conditions (C-Obs 35). 2024. https://ranzcog.edu.au/wp-content/uploads/Fetal-Anomalies-Clinical-Guideline.pdf. (last accessed August 2025).
- Centre for Genetics Education. Diagnostic tests during pregnancy. Sydney: NSW Health; 2020. Available from: https://www.genetics.edu.au/PDF/Diagnostic_tests_during_pregnancy_fact_sheet-CGE.pdf (last accessed August 2025)
- Centre for Genetics Education. Genetic services. Sydney: NSW Health; 2022. Available from: https://www.genetics.edu.au/SitePages/Genetic-Services.aspx. (last accessed August 2025).
Claim your CPD
After reading the clinical summary above and reviewing the references, complete the quiz to gain 30 minutes of EA CPD and 30 minutes of RP CPD.
You can either self-report CPD to your CPD home, or Medcast will track your learning via your personal CPD Tracker and you can download and report these points once a year. See our CPD Tracker FAQ.
Quiz
Please log in or sign up for a free Medcast account to access the case study questions and achieve the CPD credits.
Quality Use of Medicines Alliance
An evidence-based overview of perimenopause, covering common symptoms, diagnosis, lifestyle interventions, MHT prescribing principles and non-hormonal management strategies.
Medcast Medical Education Team
Eating disorders affect around 1.1 million Australians, with GPs playing a central role in early identification and coordinated care. This guide outlines Medicare pathways, including the EDTMP, Mental Health Treatment Plan and GP Chronic Condition Management Plan, along with eligibility criteria, review requirements, billing items and referral options.
Dr Nazha Nazeem
Allied health professionals play a vital role in veteran care. This guide outlines DVA card types, the allied health treatment cycle, exceptions and billing essentials – introducing allied health providers to practical knowledge that enables delivery of compliant veteran-centred care under Department of Veterans' Affairs arrangements.