
Antidepressants and youth mental health – clinical fact sheet and MCQ
Anxiety and depression in young people (aged 13–24)
Overview
Mental health conditions are a leading cause of disease burden for young Australians. Between 2020 and 2022, nearly 40% of those aged 16-24 years experienced a mental health disorder within the previous 12 months. This represents an increase in prevalence of almost 50% in the last 15 years.
- Adolescence and early adulthood are a formative time marked by significant neurobiological, psychological, and social transitions, increasing vulnerability to mental illness
- Global estimates suggest that up to 75% of mental illness emerges before the age of 25 years
- Certain groups of young people are at an increased risk of experiencing mental illness, barriers to care, and higher levels of distress. These groups include First Nations young people, LGBTIQA+ youth, young people living in rural or remote areas and from multicultural communities, and young people with disability.
Diagnosis
Clinical assessment
- When assessing young people with mental health concerns, building trust and rapport is crucial to engagement, as they may feel anxious, judged, or misunderstood in healthcare settings
- It is important to discuss confidentiality and to respect the autonomy of the young person, spending some time alone with them in the consultation where appropriate
- Limitations to confidentiality would be:
- if the adolescent is not considered to be a mature minor and/or
- there are serious concerns about risk, such as risk of harm to self or others, or suspected physical, emotional, or sexual abuse
- Diagnosis should be based on a comprehensive biopsychosocial assessment. The HEEADSSS framework is recommended to explore strengths, risks, and contextual factors, ideally over multiple consultations
- Risk assessment (including suicide and self-harm) should be conducted routinely at every visit and monitored throughout a young person’s care
- When safety plans are developed (eg, Lifeline Suicide Safety Plan), they need to be regularly revisited and reviewed
Presenting symptoms
When assessing for symptoms and signs of depression and anxiety in young people, it is important to consider that the presentation may differ across ages and developmental stages.
Young people with anxiety may present with:
- avoidance of everyday experiences and situations eg. school or social events
- frequent physical complaints eg. headache, stomach ache
- sudden emotional or angry outbursts or tantrums
- changes in sleep patterns, appetite, or weight
- being preoccupied or unable to concentrate
- overplanning and overthinking things
Young people with depression may present with:
- fatigue, reduced motivation
- poor concentration and memory
- anhedonia
- lowered self esteem
- withdrawal from others
- irritability
- changes in sleep patterns, appetite, or weight
- suicidal ideation and/or self-harm
Screening tools
Validated screening tools are recommended to help identify symptoms and severity, and to monitor progress over time, however, they are not diagnostic.
Commonly used tools include:
- DASS 21/DASS-Y – Depression Anxiety Stress Scale; DASS-Y has been validated for children and adolescents aged 7-18 years
- PHQ-9/PHQ-A – depression severity; PHQ-A is modified for adolescents aged 11-17
- GAD-7 – generalised anxiety symptoms (primarily validated for adults but also validated and used for adolescents)
- RCADS – anxiety and depression (youth-specific)
- SCARED – anxiety disorders in children and adolescents
Diagnostic criteria
Formal diagnosis is made using DSM-5 or ICD-11 criteria. Key features include:
- persistent symptoms (≥ two weeks for major depressive disorder; ≥ six months for many anxiety disorders)
- clinically significant distress or functional impairment
- symptoms not better explained by substance use, medical conditions, or normative developmental responses

Management
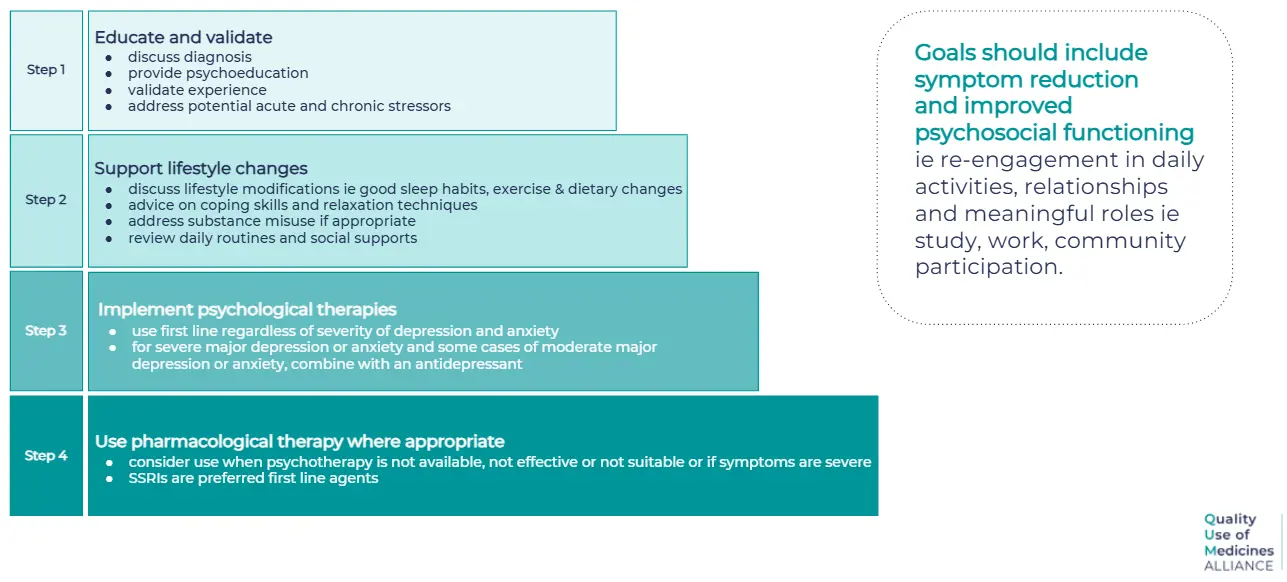
Best practice management follows a stepped-care and shared decision-making approach, matched to symptom severity, risk, and patient preference.
Non-pharmacological interventions
Lifestyle interventions (such as exercise, sleep optimisation, dietary improvements, reduction of alcohol/substance use, and social connection) are recommended for all young people living with depression and anxiety.
Psychological therapies are recommended for all severities of major depression and anxiety disorders, and as first-line treatment for mild to moderate anxiety and depression. These include:
- cognitive behavioural therapy (CBT) – strongest evidence base for both conditions
- interpersonal therapy (IPT) – particularly effective for depression
A GP mental health treatment plan can support management and enable access to subsidised psychological therapies.
Digital and blended therapies may improve affordability and accessibility when evidence based and clinician supported. A directory of reputable Australian mental health resources and services is available here.
Pharmacological management
Antidepressants have a limited and modest evidence base in young people, with high placebo response rates and small effect sizes.
It should be noted that no medications are currently licensed by the TGA for use in anxiety or depression in people <18 years in Australia.
As such, guidelines recommend reserving antidepressants for moderate to severe depression/anxiety disorders, or when psychological therapy alone is insufficient or unavailable.
- If antidepressants are deemed appropriate, selective serotonin reuptake inhibitors (SSRIs) are first-line pharmacotherapy
- Fluoxetine has more safety and efficacy data in teens and is the preferred SSRI for depression
- There is no evidence to support the use of one SSRI over another for anxiety
- Other SSRIs such as sertraline, escitalopram and fluvoxamine may be used depending on age, diagnosis, and context
- Initiate at low doses and titrate gradually
- Close monitoring is essential, particularly in the early weeks of treatment, due to risks such as activation, emerging suicidality, and unmasking of bipolar disorder
- It can take one to two weeks before improvement in symptoms and at least four to six weeks for the medication to take full effect
- Higher doses of SSRIs do not appear to improve efficacy but may increase side effects
Young people should be informed about common potential side effects, including gastrointestinal upset, headache, dizziness, fatigue, weight gain, sexual dysfunction, emotional numbing, and insomnia. Impaired judgement, reduced coordination, or drowsiness may occur for some people, so care should be taken with driving, and use of alcohol and other substances.
If medication is prescribed, it should be combined with psychological therapy wherever possible to improve outcomes.
If there is an acceptable response to antidepressants, continue at the same dose for 6-12 months, then consider de-prescribing. This resource provides more detailed information on recommended approaches to deprescribing.
It may be necessary to continue medication for longer periods in some situations (eg. recurrent depression, psychotic depression, or a serious suicide attempt).
Follow-up and referral
Regular follow-up is essential to monitor symptom response, treatment adherence, side effects, and safety. Review intervals typically range from one to two weeks initially, then monthly, with longer intervals as the young person stabilises on treatment.
Referral to specialist child and adolescent or youth mental health services is indicated for:
- severe or complex presentations
- high suicide or self-harm risk
- treatment resistance
- diagnostic uncertainty, comorbid neurodevelopmental, or substance use disorders
References
- ABS (2023) National Study of Mental Health and Wellbeing, 2020-2022. https://www.abs.gov.au/statistics/health/mental-health/national-study-mental-health-and-wellbeing/latest-release
- ABS (2008) National Survey of Mental Health and Wellbeing: Summary of Results, 2007. https://www.abs.gov.au/statistics/health/mental-health/national-study-mental-health-and-wellbeing/2007
- McGorry PD, Mei C, Dalal N, et al. The Lancet Psychiatry Commission on youth mental health. Lancet Psychiatry 2024; 11: 731–774. doi:10.1016/s2215-0366(24)00163-9
- The Royal Children’s Hospital Melbourne. Clinical Guidelines: Anxiety: identification and management. 2024. Available at: https://www.rch.org.au/clinicalguide/guideline_index/Anxiety__identification_and_management/
- Black Dog Institute. Depression in adolescents and young people. https://www.blackdoginstitute.org.au/wp-content/uploads/2022/06/Depression-in-adolescents.pdf
- American Psychiatric Association. (2022). Diagnostic and statistical manual of mental disorders (5th ed., text rev.). https://doi.org/10.1176/appi.books.9780890425787
- World Health Organization. (2019). International statistical classification of diseases and related health problems (11th ed.). https://icd.who.int/
- Malhi GS, Bell E, Bassett D, et al. The 2020 Royal Australian and New Zealand College of Psychiatrists clinical practice guidelines for mood disorders. Aust N Z J Psychiatry. 2021; 55(1): 7–1179.
- Andrews G, Bell C, Boyce P, et al. Royal Australian and New Zealand College of Psychiatrists clinical practice guidelines for the treatment of panic disorder, social anxiety disorder and generalised anxiety disorder. Aust N Z J Psychiatry. 2018;52(12):1109–72
- Therapeutic Guidelines. Melbourne: Therapeutic Guidelines Limited. Major depression. 2021. Available at: https://www.tg.org.au. (last accessed Jan 2026).
- Therapeutic Guidelines. Melbourne: Therapeutic Guidelines Limited. Anxiety and associated disorders. 2021. Available at: https://www.tg.org.au. (last accessed Jan 2026).
- Zhou X, Teng T, Zhang Y, et al. Comparative efficacy and acceptability of antidepressants, psychotherapies, and their combination for acute treatment of children and adolescents with depressive disorder: a systematic review and network meta-analysis. Lancet Psychiatry. 202l ;7(7): 581–601
- Furukawa TA, Cipriani A, Cowen PJ, et al. Optimal dose of selective serotonin reuptake inhibitors, venlafaxine, and mirtazapine in major depression: a systematic review and dose-response meta-analysis. Lancet Psychiatry. 2019; 6(7): 601–609
Claim your CPD
After reading the clinical summary above and reviewing the references, complete the quiz to gain 30 minutes of EA CPD and 30 minutes of RP CPD.
You can either self-report CPD to your CPD home, or Medcast will track your learning via your personal CPD Tracker and you can download and report these points once a year. See our CPD Tracker FAQ.
Quiz
Please log in or sign up for a free Medcast account to access the case study questions and achieve the CPD credits.
The Quality Use of Medicines Alliance is a unique consortium of health sector organisations representing quality use of medicines expertise, education providers, researchers, colleges, peak bodies, member-based organisations, and consumer groups. Funded by the Australian Government under the Quality Use of Diagnostics, Therapeutics and Pathology (QUDTP) Program.
Become a member and get unlimited access to 100s of hours of premium education.
Learn moreQuality Use of Medicines Alliance
An evidence-based overview of perimenopause, covering common symptoms, diagnosis, lifestyle interventions, MHT prescribing principles and non-hormonal management strategies.
Medcast Medical Education Team
Eating disorders affect around 1.1 million Australians, with GPs playing a central role in early identification and coordinated care. This guide outlines Medicare pathways, including the EDTMP, Mental Health Treatment Plan and GP Chronic Condition Management Plan, along with eligibility criteria, review requirements, billing items and referral options.
Dr Nazha Nazeem
Allied health professionals play a vital role in veteran care. This guide outlines DVA card types, the allied health treatment cycle, exceptions and billing essentials – introducing allied health providers to practical knowledge that enables delivery of compliant veteran-centred care under Department of Veterans' Affairs arrangements.